The President's Proposal
for Health Reform
Over the past year the
House and the Senate have been working on an effort to provide
health insurance reform that lowers costs, guarantees choices,
and enhances quality health care for all Americans. On September
9, 2009 the President laid out his principles in an address to a Joint Session of
Congress.
Building on that
year-long effort, the President has now put forth a proposal that
incorporates the work the House and the Senate have done and adds
additional ideas from Republican members of Congress. The
President has long said he is open to any good ideas for
reforming our health care system, and he looks forward to
discussing ideas for further improvements from Republicans and
Democrats at an open, bipartisan meeting on Thursday.
The proposal will make
health care more affordable, make health insurers more
accountable, expand health coverage to all Americans, and make
the health system sustainable, stabilizing family budgets, the
Federal budget, and the economy:
- It makes insurance
more affordable by providing the largest middle class tax
cut for health care in history, reducing premium costs
for tens of millions of families and small business
owners who are priced out of coverage today.
This helps
over 31 million Americans afford health care who do not
get it today - and makes coverage more affordable for
many more.
- It sets up a new
competitive health insurance market giving tens of
millions of Americans the exact same insurance choices
that members of Congress will have.
- It brings greater
accountability to health care by laying out commonsense
rules of the road to keep premiums down and prevent
insurance industry abuses and denial of care.
- It will end
discrimination against Americans with pre-existing
conditions.
- It puts our budget
and economy on a more stable path by reducing the deficit
by $100 billion over the next ten years ? and about $1
trillion over the second decade ? by cutting government
overspending and reining in waste, fraud and abuse.
Progress
この法律は、一定の条件を満たす対象者(qualified beneficiaries)に対しCOBRA 保険料を補助するという条項を含んでいる。また、この保険料の補助は、COBRA に相当する、州法で義務付けられた一定の保険加入継続プログラムにも適用される。
COBRA(Consolidated
Omnibus Budget Reconciliation Act)は、会社を辞めた人や定年退職した人とその家族が、一定期間、辞めた会社で加入していた健康保険を、同じ団体用の保険料で維持できるという法律。ただ、保険料は全額自己負担となるので、会社に勤めていた時よりも出費は
かなり増える。家族ともども健康な人なら、COBRAよりも、個人保険に加入したほうが安くなる可能性も高い。
- The Recovery Act also invests $19 billion
in computerized medical records that will help to reduce
costs and improve quality while ensuring patients’
privacy.
- The Recovery Act also provides:
- $1 billion
for prevention and wellness to improve America’s health and help
to reduce health care costs;
- $1.1 billion
for research to give doctors tools to make the
best treatment decisions for their patients by
providing objective information on the relative
benefits of treatments; and
- $500 million
for health workforce to help train the next
generation of doctors and nurses.
Guiding Principles
President Obama is
committed to working with Congress to pass comprehensive health
reform in his first year in order to control rising health care
costs, guarantee choice of doctor, and assure high-quality,
affordable health care for all Americans.
Comprehensive health care
reform can no longer wait. Rapidly escalating health care costs
are crushing family, business, and government budgets.
Employer-sponsored health insurance premiums have doubled in the
last 9 years, a rate 3 times faster than cumulative
wage increases. This forces families to sit around the kitchen
table to make impossible choices between paying rent or paying
health premiums. Given all that we spend on health care, American
families should not be presented with that choice. The United
States spent approximately $2.2 trillion on health care in 2007,
or $7,421 per person ? nearly twice the average of other
developed nations. Americans spend more on health care than on
housing or food. If rapid health cost growth persists, the
Congressional Budget Office estimates that by 2025, one out of
every four dollars in our national economy will be tied up in the
health system. This growing burden will limit other investments
and priorities that are needed to grow our economy. Rising health
care costs also affect our economic competitiveness in the global
economy, as American companies compete against companies in other
countries that have dramatically lower health care costs.
President's plan, 2009
The President's plan, and
arguments on its behalf, are available on the White House
website.
During a June 2009
speech, President Barack
Obama
outlined his strategy for reform. He mentioned electronic
record-keeping; preventing expensive conditions; reducing
obesity; refocusing doctor incentives from quantity of care to
quality; bundling payments for treatment of conditions rather
than specific services; better identifying and communicating the
most cost-effective treatments; and reducing defensive medicine.
President Obama further
described his plan in a September 2009 speech to a joint session of Congress.
His plan mentions: deficit neutrality; not allowing insurance
companies to discriminate based on pre-existing conditions;
capping out of pocket expenses; creation of an insurance exchange
for individuals and small businesses; tax credits for individuals
and small companies; independent commissions to identify fraud,
waste and abuse; and malpractice reform projects, among other
topics.
President's plan, 2010
On February 22, 2010,
President Barack
Obama
released his plan for health care reform. In his plan he outlines the key
elements on which he wants to focus. Key elements of his plan
are: policies to improve the affordability and accountability;
policies to crack down on waste, fraud and abuse; policies to
contain costs and ensure fiscal sustainability; and other policy
improvements.
On February 25 President
Obama held a Bipartisan Health Care Summit at the Blair
House.
Among the topics discussed were the rising costs of health care
and unfair insurance practices. There were several issues that
Republicans and Democrats shared agreement on, issues such as:
Preventing waste and fraud in Medicare and Medicaid; addressing
medical malpractice reform; reforming the insurance market; and
giving individuals more choices in coverage, and giving small
businesses the opportunity to pool coverage for their employees.
One on the disagreements discussed was the
call from Republicans to throw out the current bill, and start
over. President Obama said he doesn’t want to scrap a year’s worth of work and start over
saying “the millions of Americans that are
suffering can't afford another year-long debate. There's too much
at stake.”
On March 2 President
Obama sent a letter to Speaker
of the House
Nancy
Pelosi,
Senator Harry Reid, Senator Mitch
McConnell,
and Representative John
Boehner.
In the letter he referenced four Republican ideas that he thought
deserved to be explored more. Those ideas were: random undercover
investigations of health care providers that receive
reimbursements from Medicare, Medicaid, and other Federal
programs; expanding the proposed grants of $23 million to $50
million for states that demonstrate alternatives to resolving
medical malpractice disputes; increasing Medicaid payments to
doctors; and the possibility of expanding Health Savings Accounts, and making clearer language in
the President’s proposal to allow for high
deductible plans.
He also spoke of provisions in the
legislation that he felt should not be in there, such as the
Medicare Advantage provision that provided transitional extra
benefits to Florida residents, and the Nebraska FMAP provision
which would have covered that state's expanded Medicare coverage
in perpetuity.
On March 8th, in
Glenside, Pennsylvania, the president gave a speech entitled
"Fighting for Health Insurance Reform", in which he
restated the country's need for a sustainable health care system.
He explained why he believes health insurance reform is a
necessity and called on Congress to put aside politics and hold a
final up-or-down vote on reform.
Congressional proposals
Summary
of differences between proposed Health Reform Bills
| |
H.R.
3962, Affordable Health Care for America Act
"House bill" |
H.R.
3590, Patient Protection and Affordable Care Act
"Senate bill" |
| Financing |
Places a 5.4% surtax on incomes over $500,000
for individuals and $1,000,000 for families. |
Increases the
Medicare payroll tax from 1.45% to 2.35% on incomes over
$200,000 for individuals and $250,000 for families. |
| Abortion |
Insurance plans
that cover abortions (except those already allowed by the
Hyde
Amendment)
will not be eligible for federal subsidies. |
Insurance plans
that participate in the newly-created exchanges will be
permitted to include abortion coverage, but a separate
payment, not using federal funds, must be made for the
portion of the premium attributable to abortion coverage.
Each state will have the option to
exclude plans covering abortions from their insurance
exchange. |
| Public option |
Yes. |
No. Instead, the
federal government will mandate that newly-created State
insurance exchanges include at least two national plans
that are created by the Office of Personnel
Management. Of these two national
plans, at least one will have to be a private non-profit
plan. |
| Insurance
exchanges |
A single
national insurance exchange will be created to house
private insurance plans as well as a public option.
Individual states could run their own exchanges under
federal guidelines. |
Each state will
create its own insurance exchange under federal
guidelines. |
| Medicaid
eligibility |
Expanded to 150%
of the federal poverty level |
Expanded to 133%
of the federal poverty level |
| Illegal
immigrants |
They are allowed
to participate in the insurance exchanges, but cannot
receive federal subsidies. |
They cannot
participate in the exchange or receive subsidies. |
| CBO estimate of outlays |
$1,050 billion
dollars over 10 years. |
$871 billion
dollars over 10 years. |
| CBO estimate of proposal's
net effect |
Deficit would be
reduced a total of $138 billion 2010-2019 after tax
receipts and cost reductions. |
Deficit would be
reduced a total of $132 billion 2010-2019 after tax
receipts and cost reductions. |
| Takes effect |
November 22,
2010 |
December 26,
2011 |
A health insurance exchange is an organized marketplace for the purchase of health insurance set up as a
governmental or quasi-governmental entity to help insurers
comply with consumer protections,
compete in cost-efficient ways, and to facilitate the
expansion of insurance coverage to more people.
Exchanges do not bear risk themselves - they are not
insurers. Rather, they would contract with private insurers
and possibly offer a public plan option to cover specified
populations (such as those obtaining coverage through small
employers and those without employer coverage).
Currently, there are two
major proposals being considered in Congress.
On November 7, 2009, the
House passed their version of a health insurance reform bill, the
Affordable Health Care for America
Act,
220-215.
On December 24, 2009, the
Senate passed their version, the Patient Protection and Affordable
Care Act,
60-39.
The two bills are similar
in a number of ways. In particular, both bills:
- Expand Medicaid
eligibility up the income ladder (to 133% of the poverty
line in the Senate bill and 150% in the House bill).
- Establish health
insurance exchanges, and subsidize those making up to 400
percent of the poverty line
- Offer tax credits to
certain small businesses (under 25 workers) who provide
employees with health insurance
- Impose a penalty on
employers who do not offer health insurance to their
workers
- Impose a penalty on
individuals who do not buy health insurance
- Offer a new
voluntary long-term care insurance program
- Pay for new
spending, in part, through cutting Medicare
Advantage,
slowing the growth of Medicare provider payments,
reducing Medicare and Medicaid drug prices, cutting other
Medicare and Medicaid spending, and raising various
taxes.
- Impose a $2,500
limit on contributions to flexible spending accounts (FSAs), which allow for
payment of health costs with pre-tax funds, to pay for a
portion of health care reform costs.
The two bills are also
similar in that neither would have much, if any, effect on the
rising costs experienced by most Americans who currently have
private health insurance.
Additionally, the seven million Americans with FSAs above
$2,500 would see an increase in taxes due to the proposed $2,500
cap on FSA contributions.
The biggest difference
between the bills, currently, is in how they are financed. In
addition to the items listed in the above bullet point, the House
relies mainly on a surtax on income above $500,000 ($1 million
for families). The Senate, meanwhile, relies largely on an
"excise tax" for high cost 'Cadillac' insurance plans, as well as an
increase in the Medicare payroll tax for high earners.
A Cadillac plan is
defined by the U.S. Senate Finance Committee as a health
insurance
plan with yearly premiums higher than $8,000 for
individuals or $21,000 for families, but colloquially refers
to any expensive plan.
The Senate Finance Committee approved provisions that would
lump FSAs together with high-cost insurance plans and subject
them to this excise tax.
Some economists believe
the excise tax to be best of the three revenue raisers above,
since (due to health care cost growth) it would grow fast enough
to more than keep up with new coverage costs, and it would help
to put downward pressure on overall health care cost growth.
Unlike the House bill,
the Senate bill would also include a Medicare
Commission
which could modify Medicare payments in order to keep down cost
growth. According to the Department
of Health and Human Services' Centers for Medicare and Medicaid
Services,
the Senate bill would increase the share of GDP consumed by
medical spending from the current 17% to 20.9% by 2019, compared
to 20.8% under current law, primarily as a result of increased
insurance coverage under the Act, including extension of coverage
to 33 million people currently without insurance.
The bills would need to
go to Conference where differences between them may be resolved.
If the Joint Conference Committee is able to resolve any
differences between each chamber's passed version of
comprehensive health care reform, the resulting Committee Report
becomes the lead proposal and goes back to each chamber to be
voted on by the full-body. The Committee Report, if passed, can
then be presented to President Barack
Obama
for his signature into law or be vetoed back to Congress.
Congressional leaders plan to bypass submitting the bills to a
conference committee in order to expedite the process.
Differences in how each
chamber determines subsidies
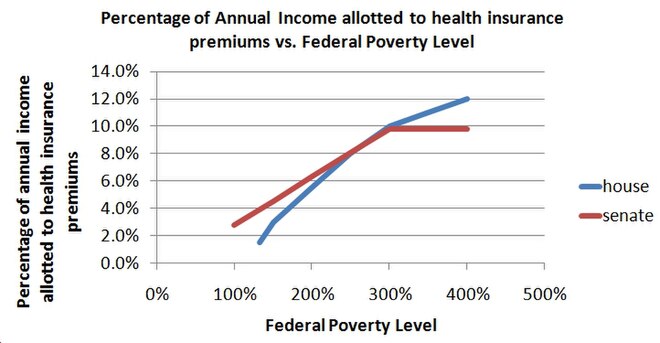
The relationship between a family's poverty level and the percentage of their
income that is allotted to pay for health insurance. Note that
the Senate Bill provides for Medicaid coverage up to 133% of the federal poverty level while the House Bill provides for
Medicaid coverage up to 150% of the federal poverty level. Adapted from the texts of the
House Bill and Senate Bill.
The
2009 Poverty Guidelines for the 48 Contiguous States and
the District of Columbia
| Persons in family |
Poverty guideline |
| 1 |
$10,830 |
| 2 |
14,570 |
| 3 |
18,310 |
| 4 |
22,050 |
| 5 |
25,790 |
How each bill determines
subsidies also differs. Each bill subsidizes the cost of the
premium and the out-of-pocket costs but are more or less generous
based on the relationship of the family's income to the federal poverty level.
The amount of the subsidy
given to a family to cover the cost of a premium is calculated
using a formula that includes the family's income relative to the
federal poverty level. The federal poverty level is related to a determined
percentage that defines how much of that family's income can be
put towards a health insurance premium. For instance, under the
House Bill, a family at 200% of the federal poverty level will spend no more than 5.5% of
its annual income on health insurance premiums. Under the Senate
Bill, the same family would spend no more than 6.3% of its annual
income on health insurance premiums. The difference between the
family's maximum contribution to health insurance premiums and
the cost of the health insurance premium is paid for by the
federal government. To understand how each bill can affect
different poverty levels and incomes, see the Kaiser
Family Foundation's
subsidy
calculator
Subsidies under House
bill
The House plan subsidizes
the cost of the plan and out-of-pocket expenses. The cost of the
plan is subsidized according to the family's poverty level, decreasing the subsidy as the poverty level approaches 400%. The
out-of-pocket expenses are also subsidized according to the poverty level at the following rates. The
out-of-pocket expenses are subsidized initially and are not
allowed to exceed a particular amount that will rise with the
premiums for basic insurance.
| For
those making between |
This much of the
out-of-pocket expenses are covered |
And no more than
this much will be spent by the individual (family) on
out-of-pocket expenses. |
| up to 150% of
the FPL |
97% |
$500 ($1,000) |
| 150% and 200% of
the FPL |
93% |
$1,000 ($2,000) |
| 200% and 250% of
the FPL |
85% |
$2,000 ($4,000) |
| 250% and 300% of
the FPL |
78% |
$4,000 ($8,000) |
| 300% and 350% of
the FPL |
72% |
$4,500 ($9,000) |
| 350% and 400% of
the FPL |
70% |
$5,000 ($10,000) |
Subsidies under Senate
bill
The Senate plan
subsidizes the cost of the plan and out-of-pocket expenses. The
cost of the plan is subsidized according to the family's poverty level, decreasing the subsidy as the poverty level approaches 400%. The
out-of-pocket expenses are also subsidized according to the poverty level at the following rates. The
out-of-pocket expenses are subsidized initially and are not
allowed to exceed a particular amount that will rise with the
premiums for basic insurance.
| For
those making between |
This much of the
out of the out-of-pocket expenses are covered |
| up to 200% of
the FPL |
66% |
| 200% and 300% of
the FPL |
50% |
| 300% and 400% of
the FPL |
33% |
The Senate Bill also
seeks to reduce out-of-pocket costs by setting guidelines for how
much of the health costs can be shifted to families within 200%
of the poverty line. A family within 150% of the FPL cannot have more than 10% of
their health costs incurred as out-of-pocket expenses. A family
between 150% and 200% of the FPL cannot have more than 20% of
their health costs incurred as out-of-pocket expenses.
The House and Senate
bills would differ, somewhat, in their overall impact. According
to Congressional Budget Office estimates, the Senate bill would
cover an additional 31 million people, cost nearly $850 billion
for coverage provisions over ten years, reduce the ten year
deficit by $130 billion, and reduce the deficit in the second
decade by around 0.25% of GDP. The House bill, meanwhile, would
cover an additional 36 million people, cost roughly $1050 billion
in coverage provisions, reduce the ten year deficit by $138
billion, and slightly reduce the deficit in the second decade
----------------------
News Week 2009/8/4
特集
米医療保険改革
オバマ政権の「国民皆保険」構想に立ちはだかるこれだけの難題
アメリカの医療保険制度は最高だ!
以前癌になった私は失業したら2度と保険に入れない、治療費が生涯限度額を超えれば保険会社は一銭も払わない、さらに悲惨な無保険者は4700万人──いったい何が問題なのか
申し訳ないが、私はアメリカの医療保険制度は現状のままでいいと思っている。私は医療保険に加入しているし、4700万人の無保険者のことなど知ったことじゃない。誰かがバラク・オバマ大統領と議会を止めるべきだ。医療改革法案を葬れ! 私は今のままのほうがトクなのだ。
「医療の公営化」に反対する手紙を大統領に出し、「私のメディケア(高齢者医療保険制度)に手を出すな」と書いた女性に私は賛成だ。メディケアが公的医療制度であることはともかく、そうこなくては!
私が連邦議員たちと同じ高水準の保障を得ていい道理などあるだろうか。法案に反対していた民主党の保守派議員などは「ブルー・ドッグ(青い犬)」と言われるだけあって顔色が悪く、たくさんの医療サービスを必要とする。私のような一般人の保障など、それより少なくて当然だ。
私は数年前に癌を患った。今の職を失えば、もう2度と医療保険には加入できないという事実を、私は気に入っている。私の住宅保険とそっくりだ。空き巣に入られたら契約を解除された。
癌の再発については考えるのも恐ろしいが、そのときに直面する究極の選択にはぞくぞくする。数十万ドルの医療費を払うために家を売るか、死ぬかの選択だ。
高額治療費を保障する保険が存在しないというのも素晴らしい。私の医療保険(結構、恵まれたものだ)は、最先端の癌治療にかかった費用の75%しか保障してくれなかった。癌で苦しみながらも自己負担の大金を支払わされる──これこそあるべき姿ではないか。
年間保険料2万5000ドルが何だ
多くの医療保険に、生涯支払い限度額が設定されているのもこたえられない。契約書の文字が小さ過ぎて見落とした人のために解説すると、保険からの医療費支払いが一定限度額を越えると、それ以上はびた一文払ってもらえないということだ。実に公平だ。
公平と言えば、どんな治療が保険の保障範囲に入るかを決めるのが医者ではなく、コスト削減を至上命題とする保険会社の事務屋たちだというのも公平に思える。何と言っても、医療のことをいちばんよくわかっているのは保険会社の連中なのだから。
そう、現状は保険会社にとって最高だ。最近知ったのだが、私たちが支払う保険料には、保険会社の事務費やマーケティング費用、利益などが手数料として含まれている。ミネソタ大学の研究によれば、保険会社の保険料収入の最大47%は医療費以外の手数料に使われている。優良な保険会社でさえ、30%近くを医療以外の目的で使っている。素晴らしい。
さらに朗報がある。企業が提供する医療保険に加入するアメリカ人は現在、1世帯当たり年間8000ドルの保険料を支払っているが、大統領経済諮問委員会によれば、25年までにはそれが2万5000ドルまで増加するという。医療保険改革の支持者はこれを「持続不可能」と言うが、そんなことはない。
そもそも、彼らはどうしたら「公的保険」などというバカげた構想を信じられるのだろう。寡占状態にある保険業界に努力を促すには競争が必要だなどと、本気で信じているのだろうか。競争を尊ぶ資本主義などという言葉があったのは大昔のことだ。
私は、営利企業である保険会社が連邦政府の資金にタダ乗りして儲ける現状こそ望ましいと思う。私たちは、企業が困ると政府が助けるという優れた福祉制度をもっている。メディケア受給者向けの処方薬を提供するプログラムを政府の代わりに運営することで、保険会社は政府から数千億ドルの手数料を受け取っている。その制度に手を触れてはいけない。腕利きロビイストが手塩にかけて作り上げた傑作を、ぶち壊しにすることになる。
議論を始めてからまだたった97年
現状のうちでも最高なのは、医者がサービス単位で支払いを受ける仕組みだ。医者は、処置の一つ一つに対して支払いを受ける。自動車販売員が、車を売った対価ではなく、ハンドルを握ったりブレーキを踏んだりするたびにコミッションを受け取るようなものだ。近所のショッピングセンターで開業しているクリニックの医療のほうが、医者が給与ベースで働いているメイヨー・クリニックやスローン・ケタリング記念癌センターなどの大病院よりはるかに優れているのもそのおかげだ。誰がこのシステムを壊したがるだろうか。
よろしい、認めよう。私も本音では変化を望んでいる。自分たちも「改革者」だと言うために共和党議員が持ち出した政策を、私は支持する。彼らによれば、医療過誤訴訟で認める損賠賠償支払い額に上限さえ設ければ、医療保険制度全体を救うことができる。カリフォルニア州とテキサス州という全米最大の2つの州が数年前にその通りのことを実施したが、何も良くならなかった。だが、誰がそんなことを気にするだろう。何より、この政策は聞こえがいい。
だから、米議会が夏休みになって地元の議員が帰ってきたら、医療保険改革はまだ時期尚早だと訴えよう。何せ、私たちがこの議論を始めてからまだ
97年しか経っていない。1912年にセオドア・ルーズベルトが革新党の選挙公約に公的医療保険を掲げたのが最初だからだ。議会の公聴会もたった745回しか開かれていない(ちゃんと数えたわけではないが)。こんなものではとても足りない。何かをする前に、もっとこの問題を研究しよう。
たった今、私は「問題」と言ったか? 問題など何もない。私は現状維持が好きなのだ。
